By Fabian Poletti MD, MSc (DIC), FRCS (Eng), FEBOT (T&O) Consultant Orthopaedic and Trauma Surgeon
Inside the Mind of a Fighter: Why This Patient Is Different
As an orthopaedic surgeon with years of experience treating athletes from various disciplines, I’ve come to understand that combat athletes—wrestlers, boxers, BJJ practitioners, MMA fighters—do not follow the traditional rules of sports medicine. They redefine them.

These are not mere sportspeople; they are warriors whose relationship with pain, trauma, and physical intensity stands apart from the high-performance athlete archetype. And yet, most treatment protocols continue to view them through the same lens as a marathoner or a football player. This is a clinical oversight I believe must change.
Before becoming a surgeon, I too was an athlete. My background is in track and field, where performance is defined by precision, biomechanics, and timing. While my foray into combat sports was driven more by a deep personal passion for martial arts—especially aikido and kickboxing—it gave me firsthand insight into the mindset of the fighter: the discipline, the ritual, and the singular way in which these athletes relate to pain, body, and movement.
Over the years, I’ve had the privilege—and the responsibility—of treating fighters who redefine the boundaries of human resilience. Not weekend warriors or casual practitioners, but professional and dedicated amateur combat athletes: boxers, wrestlers, jiu-jitsu black belts, Muay Thai warriors, MMA gladiators. Men and women who step onto the mat or into the cage not in perfect condition, but already broken—and yet, still fighting.
I’ve seen anterior cruciate ligaments torn and left unrepaired for months, even years, while their owners kept drilling takedowns. I’ve treated shoulders with labral tears so extensive that any ordinary person would have been unable to lift a glass—yet these fighters continued throwing punches at full force. I’ve diagnosed advanced, bone-on-bone osteoarthritis in knees that still bent into full guard. Some came to me with stress fractures that had long passed the stage of pain and entered the realm of structural collapse. In some, we discovered chronic avulsion injuries, subchondral oedema, or partial tendon ruptures that had gone completely undiagnosed, masked by a psychological threshold for pain most people can’t even imagine.
But what stops these fighters—if anything ever does—is not the pain. Pain, for them, is just another sparring partner: acknowledged, managed, compartmentalized. They’ve trained through hematomas, through joint effusions, through burning nerve pain. What truly brings them to their knees—often literally—is not suffering, but dysfunction. The inability to rotate the hip, extend the elbow, or plant the foot with precision. It’s the creeping rigidity of synovial inflammation that blocks their rhythm, the swelling that kills their timing, the mechanical block that makes their signature move no longer executable. They don’t quit because they hurt—they pause when they can no longer perform. And that, in the world of combat sports, is a far more devastating injury.
The Profiles Behind the Warriors: Typologies of the Combat Athlete
The Grappler: Isometric Warfare and Silent Swelling
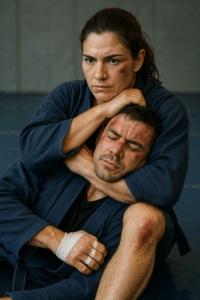
Grapplers are the technicians of joint manipulation. They fight with leverage, torque, and constant isometric control. Their world is one of hyperflexion, rotational overload, and constant axial compression. The knees are subjected to valgus forces in positions of deep flexion, while the lumbar spine absorbs shock from repeated takedown impacts. In BJJ, long training sessions on the mat result in chronic joint effusions, meniscal degeneration, and bone marrow lesions, particularly in the posterior femoral condyle and tibial plateau.
In many grapplers I’ve treated, persistent joint swelling becomes normalized, and their main concern is whether they can finish a sweep, lock a triangle, or invert under pressure. What would sideline a footballer or runner for weeks is simply part of the routine for them. But when the joint loses its end-range mobility—when inflammation narrows the arc of control—that’s when performance drops.
The Striker: The Silent Breakdown in the Precision Athlete
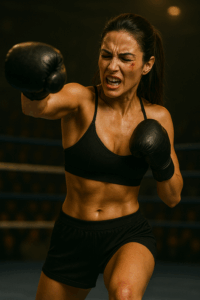
Boxers are explosive athletes. Every punch is a kinetic chain from foot to fist, requiring pristine coordination of the ankle, hip, thorax, scapula, elbow, and wrist. But repeated microtrauma—often thousands of impacts per training week—leads to gradual structural decay. I’ve treated boxers with CMC joint collapse, carpal instability, rotator cuff tendinosis, and labral tears, many of which go unnoticed until performance falters.
Unlike grapplers, boxers worry less about swelling and more about precision and timing. A one-degree loss in shoulder external rotation or wrist stability might not cause pain, but it can translate to a missed hook or decreased knockout power. The treatment must target biomechanical restoration, not just symptom suppression.
Their central nervous system is also uniquely conditioned. Chronic sub-concussive trauma modifies neuroplasticity, reaction time, and autonomic tone. While this is often outside the scope of orthopedic care, it reinforces the need to maintain structural harmony so the boxer can continue to train without compromising cognitive health.
The Kicker: Strike, Absorb, Endure

Strikers in Muay Thai and Kickboxing present a distinct biomechanical pattern: repetitive impact loading to the lower extremities, rotational stress at the hips and knees, and shearing forces through the lumbar spine and pelvis. Unlike traditional boxers, kickers use their legs as both weapon and shield—delivering and absorbing strikes with shins, knees, and even the instep.
Common injuries include chronic periostitis, stress reactions in the tibia and metatarsals, hip labral injuries, and ankle impingement syndromes from repeated high-velocity dorsiflexion. In many of these athletes, the tibial cortex adapts through sclerosis and cortical thickening, but when microfractures accumulate, the risk of overt stress fracture rises.
The hips and knees are especially vulnerable—particularly from constant pivoting on the support leg during rotational strikes. As a knee surgeon, I often see early cartilage degeneration and bone marrow oedema in these patients. Many continue training until their kick “feels soft” or their shin “stings too long.” The goal of treatment is not simply to reduce pain, but to restore impact confidence—an entirely different metric than standard pain scales.
The Hybrid Fighter: Polytrauma in Transition

Mixed Martial Artists live in a zone of constant adaptation. They must throw powerful leg kicks, sprawl, clinch, shoot, and scramble—often within the same round. The result is a polytraumatized athlete. I’ve seen fighters with past AC joint separations, partially healed rib fractures, PCL injuries, and ankle instability, all coexisting within a single kinetic chain.
The main issue in MMA patients is cumulative overload without centralized symptoms. They don’t come in complaining of one joint; they come in because “everything feels off.” These are athletes who can no longer maintain rhythm during a transition or feel “heavy” when switching stances. Evaluation reveals subtle joint effusions, regional swelling, and kinetic compromise. The knee often presents with nonspecific tightness, loss of proprioception, or mechanical stiffness—not dramatic findings, but enough to disrupt transitions in a high-level fight.
Why Traditional Treatment Fails?
Rehab is Not Exile – Rethinking Recovery for the Warrior Patient
Ask a combat athlete to complete rest for four weeks, and you’re not simply interrupting a training cycle—you’re dismantling a psychological framework that holds their entire identity together. You’re not prescribing rest; you’re prescribing exile. For fighters, the mat is not a place—it’s a state of being. The sound of gloves striking pads, the sweat-soaked silence after a sparring round, the ritual of taping hands and stepping barefoot into the cage—these are not accessories to life; they are life.
To remove a fighter from that environment in the name of “healing” without understanding what you’re truly disrupting is not just naïve—it’s clinically negligent. The training-induced cascade of neurochemicals—endorphins, dopamine, serotonin—is not a luxury; it is their psychological scaffolding. For many of these athletes, especially those with traumatic backgrounds, combat sports are their therapy, their discipline, their self-worth condensed into a daily structure. Take that away for a month, and you don’t get recovery—you get withdrawal. Anxiety rises, mood deteriorates, eating and sleeping rhythms collapse, and the risk of non-compliance skyrockets.
Traditional rehabilitation protocols, with their staged timelines, isolated exercises, and emphasis on progressive loading divorced from real-world context, often fail miserably when applied to this population. They ignore the cultural, emotional, and neurobiological reality of the combat athlete. Healing, in this arena, cannot be synonymous with detachment.
What’s needed is a fundamentally different paradigm—a biologically integrative recovery protocol that respects the unique physiology and psychology of the fighter. One that blends cutting-edge regenerative medicine with a training-conscious framework. We must move beyond the binary of rest versus reinjury and embrace strategies that allow for active regeneration.
My personal Approach: Biologic Precision for the Warrior Patient: Regenerative Medicine in Combat Sports

Combat athletes challenge anatomy with a unique frequency, intensity, and disregard for conventional recovery logic. That’s why orthobiologic strategies must evolve—not only to meet biomechanical demands but to match psychological rhythms. In my clinical approach, I’ve adopted a precision-based model tailored to individual pathology, fighting style, and load tolerance—not generalized recovery timelines.
As a knee surgeon, I pay particular attention to the kinetic chain stressors that define striking, grappling, and hybrid combat disciplines. The knee—constantly rotating under load, absorbing axial shocks, and transitioning from flexion to hyperflexion—is often the first joint to show degenerative changes in fighters. It’s also the joint most crucial for stance stability, takedown mechanics, sprawl, and lateral movement. In this context, orthobiologic precision is not optional—it’s foundational.
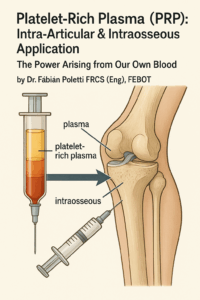
Platelet-Rich Plasma (PRP): Intra-Articular & Intraosseous Application
The Power Arising from Our Own Blood
In the world of combat sports, healing must be proactive. Over the years, I’ve shifted from symptom suppression to structural preservation—especially in knee pathology, which remains the cornerstone of function in all fighting styles. Cartilage degeneration, subchondral overload, meniscal dysfunction, or persistent effusion must be managed with biologics not as an afterthought, but as a frontline strategy.
PRP remains central to my regenerative protocol, especially in combat athletes with subclinical or advanced degenerative joint changes. I employ high-volume PRP in two distinct modes:
- Intra-articular PRP (IA-PRP): Modulates synovial inflammation, restores joint homeostasis, and protects cartilage by leveraging key growth factors—PDGF, TGF-β, VEGF, and IGF-1. This is particularly effective in fighters with chronic effusions, early cartilage softening, bone-on-bone arthritis, and post-traumatic inflammation. In this population, the goal is often functional restoration more than pain relief.
- Intraosseous PRP (IO-PRP): Targets bone marrow lesions, subchondral oedema, and trabecular microfractures—common findings in the knees of strikers and wrestlers exposed to repeated torsion, pivoting, and impact trauma. IO-PRP is also considered in advanced osteoarthritis with focal edema or structural overload, particularly when surgery is to be postponed. In selected cases, subchondroplasty is combined to address early stress fractures and restore mechanical integrity.
Whenever IO-PRP is indicated, I often combine it with diagnostic arthroscopy, not just to visualize the joint but to address mechanical irritants—such as hypertrophic synovium, loose bodies, or unstable cartilage flaps—that could compromise the regenerative response. This combined mechanical-biological reset allows for early return to sport with reduced dysfunction.
PRP is also effective in:
- Chronic patellar tendinopathy and quad tendinopathy
- Muscle injuries in the quadriceps or hamstrings
- Early and late-stage osteoarthritis
- Post-surgical joint stiffness or inflammatory flare-ups
Its autologous nature ensures safety, and in the right context, PRP can delay or even avoid surgical interventions—preserving athletic careers while maintaining tissue integrity.
⚠️ I strictly avoid PRP in patients with active infection, neoplastic disease, uncontrolled bleeding disorders, severe anemia, or systemic autoimmune flare.
As part of a truly integrative treatment plan, these biologics are most effective when supported by a broader therapeutic strategy that may include anti-inflammatory nutrition, targeted supplementation, restorative sleep protocols, and even mindfulness-based stress reduction—tools that respect the athlete’s physiology and psychology alike without diluting the clinical focus.
Hyaluronic Acid (HA): Restoring Viscosity and Confidence
Often underestimated, HA injections play a pivotal role in my treatment of fighters—particularly in managing low-grade synovitis, post-impact inflammation, and friction-related discomfort in the knee. Unlike passive patients, combat athletes benefit from viscoinduction, not just mechanical lubrication.
I select HA formulation and dosage based on:
- Molecular weight: High-weight options for prolonged effect
- Combination protocols: HA + PRP when synergistic modulation is needed in moderate/advance OA
In my experience, HA is especially useful in patellofemoral syndrome in grapplers and kickers. Clinical benefits include improved motion arcs, reduced effusion recurrence, and enhanced proprioception—critical for fighters who rely on precise stance and transitional explosiveness.
Corticosteroids: Rare, Restrained, and Reserved
My stance on corticosteroids is unequivocal: I avoid them unless absolutely necessary.
Intra-articular corticosteroids, while effective in rapidly suppressing inflammation, carry well-documented risks—particularly chondrotoxicity, collagen degradation, and masking of underlying injuries. These risks are magnified in combat athletes who may return to high-impact training prematurely.
That said, there are exceptional circumstances where a single, low-dose corticosteroid injection may be justified:
- Severe reactive synovitis unresponsive to conservative management
- Acute OA flare-ups threatening short-term functional participation
- Pre-competition crisis scenarios where all other options are exhausted
Even then, corticosteroids are employed with caution, transparency, and time-bound planning, always as a bridge—not a solution. My guiding principle is long-term joint preservation, not temporary suppression of symptoms.
Responsible Regenerative Medicine in Fighters
I reject the commodification of orthobiologics. There are no cookie-cutter protocols in my practice—only bespoke treatment plans informed by:
• Detailed clinical evaluation
• Imaging-guided diagnosis
• Biomechanical insight
• And surgical backup, when necessary
Each case is mapped in terms of function, urgency, and career trajectory. The art lies in knowing not just how, but when to intervene. Poorly timed injections can delay surgery and compromise healing. Properly indicated ones can extend careers, optimize tissue quality, and buy time for surgical planning without halting training entirely.
As a surgeon, I don’t view orthobiologics as an alternative to surgery. I view them as part of a strategic continuum—sometimes a detour, sometimes a delay, sometimes an accelerator. The key is alignment with clinical goals, patient psychology, and athletic realities.
Why Fighters Choose This Approach
In a landscape saturated with commercial PRP clinics and generic sports rehab centers, my model offers something different: care rooted in surgical understanding, athletic empathy, and scientific rigor.
I don’t just inject—I assess. I ask about stance switches, takedown speed, guard transitions, leg kicks, and pain thresholds. I look at radiographs, yes—but also at the way a fighter steps into the clinic. Because often, the dysfunction starts before the MRI shows it. Every action I take is tied to performance, not just pathology.
Final Thoughts
Combat athletes don’t ask to be pain-free.
They ask to keep going.
And my responsibility is not simply to heal tissue. It’s to protect momentum—to keep the fight alive, not just in the octagon or on the mat, but in the heart of the athlete.
This isn’t just regenerative medicine.
This is high-stakes preservation of identity, power, and purpose.
Learn more at drpoletti.com
Leave a Reply