By Fabian Poletti MD, MSc (DIC), FRCS (Eng), FEBOT (T&O) Consultant Orthopaedic and Trauma Surgeon
Peptides occupy a paradoxical position in modern medicine. On the one hand, they are among the most successful therapeutic molecules ever developed. Insulin fundamentally altered the prognosis of diabetes. GLP-1 receptor agonists have reshaped the management of type 2 diabetes and obesity, becoming some of the most impactful—and profitable—drug classes in modern medical history. Growth hormone analogues, calcitonin, parathyroid hormone derivatives, gonadotropin-releasing hormone (GnRH) analogues, and multiple oncologic and rare-disease therapies are all peptide-based.
In simple biological terms, peptides are short chains of amino acids—smaller than full proteins—that function as signalling molecules, regulating processes such as metabolism, inflammation, tissue repair, and hormonal communication throughout the human body.
On the other hand, in orthopaedics and sports medicine, peptides such as BPC-157, TB-500, and others frequently referenced in popular culture and online communities remain firmly outside the boundaries of regulated clinical practice. Despite their widespread use and frequent discussion among patients, these compounds are almost entirely unsupported by robust human safety data.
This disconnect has created a large and uncomfortable clinical vacuum—one that many clinicians choose to ignore, but one that increasingly affects every day orthopaedic decision-making.
Biological plausibility is not the problem
It is important to state clearly, from the outset, what this discussion is not.
The absence of regulatory approval for most peptides currently used in orthopaedic and sports-medicine contexts does not imply that peptides as a class are ineffective, unsafe, or scientifically unserious. Quite the opposite. Medical history repeatedly demonstrates that peptides, once properly studied and validated, can become cornerstone therapies.
Insulin is a peptide.
GLP-1 receptor agonists are peptides.
Parathyroid hormone analogues are peptides.
Paraphrasing a sentiment often expressed in public discourse, “history teaches us that many peptides initially viewed with scepticism later proved to be transformative once rigorous science caught up with biological plausibility”. It is therefore entirely reasonable—at least from a mechanistic and physiological standpoint—to assume that some of the peptides currently circulating in orthopaedic and sports-medicine settings may exert meaningful biological effects.
However, plausibility is not permission.
In medicine, biological plausibility alone is insufficient to justify clinical use. Between a plausible mechanism and a defensible therapy lies a structured process of toxicology, pharmacokinetics, human safety assessment, and regulatory oversight. It is precisely this process—not scepticism toward peptides themselves—that defines the current impasse.
The physician’s constraint: ordered validation
Medicine does not advance through intuition, popularity, or anecdote.
It advances through ordered validation.
As physicians, we are ethically, legally, and professionally bound to follow a defined sequence before any compound can be considered safe for clinical use:
- Preclinical toxicology: to identify systemic and target-organ risk
- Pharmacokinetic and dose–exposure characterization: to understand biological behaviour
- Controlled human safety studies: to define tolerability and risk
- Only then efficacy and clinical integration
For this reason, physicians cannot decide that a compound is acceptable simply because:
- Many patients are already using it
- The mechanism appears biologically plausible
- Anecdotal outcomes seem favorable
History is filled with examples where all the above were true—and patients were harmed.
The fact that a substance is widely used does not make it safe.
The fact that it “makes sense” biologically does not make it harmless.
The fact that some patients report benefit does not establish an acceptable risk profile.
This is not conservatism.
It is the framework that prevents harm.
The reality in orthopaedic practice
In real-world orthopaedic and sports medicine clinics, peptides are no longer rare or fringe.
In my own clinical practice as an orthopaedic surgeon, approximately 20–30% of patients openly report having used, currently using, or actively considering the use of peptides. This figure reflects only those patients who acknowledge such use.
Based on clinical experience, it is highly likely that the true prevalence is higher, as many patients do not disclose peptide use unless specifically asked—and often only after a relationship of trust has been established. This pattern is particularly evident among younger, athletic, and physically active individuals, who represent a substantial proportion of sports orthopaedic practice.
This creates an unavoidable clinical reality.
I cannot prescribe these compounds.
I cannot endorse them.
But I cannot pretend they are not part of my patients’ therapeutic landscape.
From a clinical standpoint, this is deeply unsatisfactory. Ideally, emerging therapies with biological plausibility and widespread use would be studied, regulated, monitored, and integrated into care, allowing physicians to guide patients rather than observe from the sidelines.
At present, however, this is not possible.
The only defensible position is to remain informed, attentive, and transparent—acknowledging potential biological interest, clearly stating the limits of current evidence, and continuing to base medical decisions on validated treatments and established safety frameworks.
Ignoring this reality does not protect patients.
Engaging with it responsibly, even within strict constraints, is the minimum requirement of good clinical practice.
The dangerous interaction gap
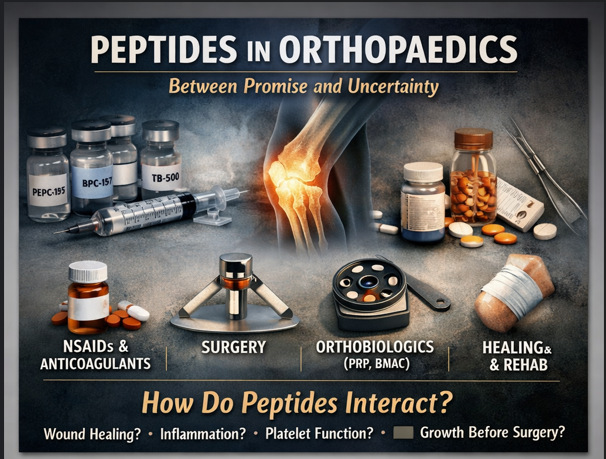
The most significant risk surrounding the widespread, unregulated use of peptides in orthopaedic and sports medicine is not limited to the peptides themselves. It lies in the unknown interactions between these compounds and the treatments we routinely prescribe.
Patients who use peptides are often, simultaneously:
- Undergoing surgical procedures
- Taking non-steroidal anti-inflammatory drugs (NSAIDs) or anticoagulants
- Receiving corticosteroids
- Undergoing orthobiologic treatments such as platelet-rich plasma (PRP), bone marrow aspirate concentrate (BMAC), or hyaluronic acid
- Engaged in structured rehabilitation protocols
In this context, the absence of human data creates a clinically relevant blind spot.
At present, we do not know:
- Whether certain peptides interfere with surgical wound healing
- Whether they alter inflammatory cascades in ways that help or hinder tissue repair
- Whether they modulate platelet activation, aggregation, or growth-factor release
- Whether they amplify, blunt, or unpredictably distort the effects of orthobiologic therapies
- Whether perioperative continuation or discontinuation affects outcomes or complication rates
These are not theoretical concerns. They are practical questions that arise daily in clinical decision-making.
Why this matters in orthopaedics
Orthopaedic interventions—whether surgical or biological—depend heavily on controlled inflammation, timely angiogenesis, and coordinated tissue remodeling. Even subtle modulation of these processes can shift outcomes in either direction.
Introducing biologically active compounds into this environment, without understanding their interactions, introduces variability that clinicians cannot account for. When outcomes are suboptimal, we are left without the tools to determine whether peptides played no role, a beneficial role, or a harmful one.
This uncertainty undermines:
- Perioperative planning
- Interpretation of treatment response
- Postoperative complication analysis
- The reproducibility of clinical outcomes
The silent confounder
Perhaps most concerning is that peptide use often remains undisclosed unless specifically elicited. This means peptides may act as a silent confounder in both clinical practice and outcome assessment.
When a patient experiences:
- Unexpected healing patterns
- Atypical inflammatory responses
- Variable response to orthobiologic injections
- Delayed recovery or unexplained complications
The clinician is left interpreting these outcomes in the absence of a complete pharmacological picture.
This is not merely an academic concern. It directly affects clinical judgment, patient counselling, and the refinement of treatment protocols.
The cost of not knowing
The absence of data forces clinicians into one of two suboptimal positions:
- Ignore peptide use entirely, treating it as irrelevant
- Overreact to uncertainty, advising blanket discontinuation without evidence
Neither approach is defensible.
The first minimizes a potentially relevant variable.
The second introduces arbitrary decision-making unsupported by data.
What is missing is measured, structured knowledge—knowledge that allows clinicians to stratify risk, adjust timing, and integrate or exclude interventions rationally.
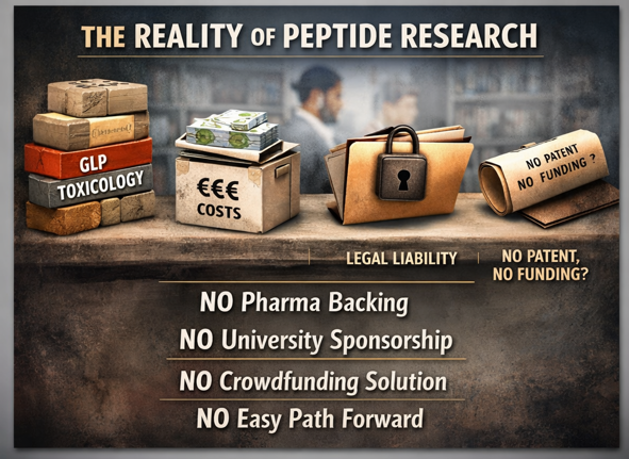
A preventable problem
This interaction gap exists not because it is scientifically uninteresting, but because it sits at the intersection of:
- Non-patentable compounds
- High regulatory barriers
- Diffuse responsibility
- Widespread real-world use
It is precisely this type of gap that public health–oriented research is meant to address.
Until it is addressed, clinicians will continue to practice in partial darkness—aware of a variable that may matter, yet unable to quantify or manage it effectively.
That is not innovation.
It is uncertainty by omission.
Given the clinical relevance of these unanswered questions, a natural response would be to ask why such interactions have not been properly studied. The answer, however, is not indifference or lack of interest—it is structural impossibility.
Why “just doing a study” is not realistic
Patients and non-clinicians frequently ask a seemingly reasonable question:
Why don’t doctors simply study these peptides properly?
At first glance, the question appears logical. If peptides are biologically active, widely used, and increasingly present in orthopaedic and sports medicine practice, why has formal clinical research not kept pace?
The answer is not lack of interest, intellectual resistance, or professional inertia.
It is structural impossibility within modern regulatory systems.
In places with a strong tradition of biomedical research—the European Union, the United States, and the United Kingdom—clinical research operates within closely aligned regulatory frameworks. While details differ, the underlying principles are shared: human exposure to biologically active compounds requires prior demonstration of safety through a defined, sequential process.
In Europe, this process is governed by the EU Clinical Trial Regulation.
In the United States, by FDA IND requirements.
In the United Kingdom, by MHRA frameworks, which remain closely harmonised with international standards.
Across all three systems, a legitimate first-in-human safety study requires, at a minimum:
- Full GLP toxicology in two animal species, including acute, sub-chronic, and target-organ toxicity
- Detailed pharmacokinetic and dose–exposure studies, to establish systemic exposure and biologically active concentrations
- GMP-grade manufacturing and stability testing, ensuring pharmaceutical-quality consistency
- Formal regulatory authorisation, with ethics committee approval
- An identifiable sponsor, legally and financially responsible, carrying insurance and full liability for adverse outcomes
These requirements are not optional, and they are not negotiable based on enthusiasm, popularity, or perceived safety.
The real cost of compliance
The consequence of this framework is cost.
Completing a compliant preclinical and early human safety programme for a single peptide, before any efficacy is explored, typically requires €15–30 million (or the equivalent in USD or GBP). This figure reflects:
- GLP toxicology packages
- GMP manufacturing
- Regulatory submissions
- Phase I safety trials
Crucially, this investment is required before answering whether the compound works, whether it offers clinical benefit, or whether it should ever be used at scale.
For individual clinicians, academic departments, or even most professional societies, this level of funding is simply unattainable.
Why GLP-1 peptides could be studied — and others cannot
GLP-1 receptor agonists are often cited as evidence that peptides can successfully navigate this pathway. This is correct—but frequently misunderstood.
GLP-1 did not succeed because it was a peptide.
It succeeded because the economic and structural conditions allowed the science to be done.
The GLP-1 story involved:
- Over 30 years of cumulative biological research
- An estimated $500 million to $1 billion to bring the first GLP-1 drug to market
- Billions more for second-generation molecules, cardiovascular outcome trials, and obesity indications
For example, the cumulative investment by industry in semaglutide across diabetes and obesity indications alone is estimated to exceed $2–3 billion.
This level of investment was rational because GLP-1 compounds were:
- Patentable
- Linked to clear, chronic disease indications
- Supported by massive market potential
The regulatory burden was enormous—but the incentive structure justified absorbing it.
The patent paradox
Most peptides currently circulating in orthopaedic and sports medicine contexts exist in a fundamentally different economic reality.
They are not meaningfully patentable, or offer only weak, easily circumvented protection. Without patent protection:
- There is no exclusivity
- There is no predictable return on investment
- There is no rational incentive for pharmaceutical companies to fund €15–30 million safety programmes per compound
As a result, industry disengagement is not ideological. It is economically rational.
This is not a moral failure of pharmaceutical companies.
It is a structural limitation of the current system.
Why academic medicine cannot fill the gap
It is tempting to assume that universities, teaching hospitals, or publicly funded academic groups could step in where industry does not.
In practice, this is rarely feasible.
Academic institutions in Europe, the United States, and the United Kingdom operate under the same regulatory and liability frameworks as industry. They must still:
- Comply with GLP and GMP standards
- Secure regulatory authorisation
- Identify a legal sponsor
- Accept full liability for adverse events
Without industry-level funding or government-level backing, academic groups simply cannot absorb this risk.
Why crowdfunding and public donations fail
Public enthusiasm and crowdfunding are often proposed as alternative solutions.
However, crowdfunding can distribute money, but it cannot distribute responsibility.
Any human clinical study still requires:
- A legally accountable sponsor
- Insurance coverage
- Regulatory oversight
- Acceptance of liability if harm occurs
Moreover, research whose most likely outcome may be “this compound should not be used” is fundamentally misaligned with donor psychology. Even well-intentioned public funding struggles to sustain projects designed to restrict or invalidate widely used substances.
As a result, crowdfunding is not a realistic pathway for first-in-human peptide safety research.
Not indifference — but systemic mismatch
The absence of clinical studies on peptides in orthopaedics and sports medicine is often misinterpreted as professional disinterest or excessive conservatism.
In reality, it reflects a systemic mismatch between four forces that do not align:
- Widespread real-world use
- High regulatory thresholds
- Lack of meaningful patentability
- Absence of a viable funding mechanism
Clinicians recognise the problem.
Regulators recognise the risk.
Industry recognises the lack of incentive.
What is missing is not awareness, but a structural pathway capable of addressing public-safety questions when traditional drug-development models are not applicable.
The unavoidable consequence
The inability to “just do a study” does not freeze reality.
Patients continue to use peptides—often chronically, often in combination with prescribed treatments, and frequently without structured medical supervision.
Clinicians continue to encounter this use, yet remain professionally and legally constrained, limited to documentation, cautious counselling, and informal risk assessment.
Regulators continue to require levels of evidence that, under the current economic and legal framework, cannot realistically be generated.
Industry continues to abstain, as these compounds are largely non-patentable, lack exclusivity, and offer no predictable return on investment. The absence of research does not represent neutrality. It represents unacknowledged exposure.
From stalemate to clinical condition
Taken together, these dynamics ensure that a clinically relevant problem does not remain static, but instead evolves into a persistent, system-wide evidence vacuum.
This vacuum actively shapes clinical behaviour, increases variability in outcomes, and forces clinicians to make decisions in the absence of data that would normally be considered essential. While administratively convenient for institutions and economically rational for industry, it is not benign for patients.
This is not merely a regulatory stalemate.
It is a clinical condition.
Ignoring this reality may be easy.
But ease should not be confused with responsibility.
Comfort is not a substitute for good medicine.
Why this vacuum matters specifically in orthopaedics and sports medicine
The relevance of peptides in orthopaedics and sports medicine is not accidental, nor driven by novelty. It is driven by clinical demand.
In this field, peptides are predominantly used by patients in an attempt to address:
- Degenerative joint disease and osteoarthritis
- Chronic musculoskeletal pain and inflammatory syndromes, including mechanical low back pain
- Tendinopathies and enthesopathies, particularly when refractory to conventional management
- Overuse-related pathology in athletic and physically active populations
- Acute musculoskeletal trauma, involving muscle, tendon, and ligament structures, especially when recovery is delayed or incomplete
These conditions are not marginal. Musculoskeletal disorders represent one of the largest disease burdens worldwide, and are among the leading causes of chronic pain, disability, loss of productivity, and long-term healthcare expenditure.
From a public health perspective, this is not a niche domain. It is an epidemic.
The cost of current standard care
Pain and inflammation in musculoskeletal disease are still predominantly managed with:
- Non-steroidal anti-inflammatory drugs (NSAIDs)
- Analgesics
- Corticosteroids
- In selected cases, opioids
While often effective in the short term, these therapies carry a well-documented systemic cost.
Chronic or recurrent NSAID exposure is associated with:
- Gastrointestinal bleeding
- Renal dysfunction
- Cardiovascular risk
- Increased perioperative complications
Globally, complications related to NSAID use account for millions of adverse events each year, substantial mortality, and enormous direct and indirect healthcare costs. These complications disproportionately affect the same populations suffering from chronic musculoskeletal pain.
It is within this context—not ideology, not trend-following—that patients seek alternatives.
In orthopaedics and sports medicine, patients are rarely pursuing performance enhancement. They are seeking pain control, functional recovery, and reduction in long-term pharmacological burden.
Why the evidence gap becomes a public health problem
The absence of evidence does not imply absence of effect.
It implies absence of knowledge.
When large populations are exposed—often repeatedly and chronically—to biologically active compounds for conditions that are:
- Highly prevalent
- Disabling
- Costly to healthcare systems
- Suboptimally addressed by existing therapies
Then the absence of structured safety and interaction data ceases to be an academic inconvenience. It becomes a public health problem.
In practical terms, this means that:
- Clinical outcomes become harder to interpret
- Variability increases without explanation
- Interactions with surgery, pharmacology, and orthobiologics remain invisible
- Complications and unexpected responses lack proper context
This is not a theoretical concern.
It is a daily clinical reality in orthopaedic and sports medicine practice.
A familiar pattern: when public health, not the market, carried the burden
This situation is not unprecedented in medicine.
There are well-established examples where critical areas of patient safety and population health were addressed not because they were profitable, but because they were necessary.
Vaccination programs for low-profit or neglected diseases advanced largely through public funding and international collaboration long before commercial incentives existed. Antibiotic research and stewardship initiatives increasingly rely on public investment as market incentives collapsed, despite the existential threat of antimicrobial resistance. Large-scale registries, surveillance systems, and post-marketing safety studies have repeatedly been funded by governments and public institutions precisely because industry could not justify the cost.
In each case, the logic was consistent:
When exposure is widespread and the cost of ignorance is borne by society, research becomes a public responsibility.
The current situation surrounding peptide use in orthopaedics and sports medicine follows this same pattern.
When the market fails, public health must intervene
The core issue, therefore, is not lack of scientific interest or biological plausibility.
It is a structural failure of the market to address a public safety issue.
Pharmaceutical companies act rationally when they decline to invest tens of millions of euros into compounds that:
- Cannot be patented
- Offer no exclusivity
- Carry significant regulatory and reputational risk
But rational market behavior does not always align with public health priorities.
When exposure is widespread, interactions are unknown, and downstream complications are absorbed by healthcare systems, inaction itself becomes a public health decision.
A call to action: shared responsibility
This is precisely the domain where medical societies, public health systems, and supranational research frameworks must assume leadership.
Organizations such as ESSKA, the American College of Sports Medicine, and related orthopaedic and sports medicine societies are uniquely positioned to define research priorities, coordinate multicenter efforts, and frame clinically relevant questions—without promoting or endorsing unvalidated therapies.
Likewise, national public health systems, research councils, and large-scale European research programs supported by the European Commission are the only actors capable of funding research whose primary return is safety, clarity, and standardization, rather than profit.
The objective is not approval or endorsement.
The objective is to:
- Fund independent safety and interaction studies
- Support large observational registries capturing real-world use
- Clarify perioperative management (when to stop, when not to stop)
- Identify clear red flags where harm is likely
- Reduce unjustified variability in clinical decision-making
These are exactly the domains where public investment is justified, because the benefit is collective and the cost of ignorance is systemic.
The cost of continued inaction
Ignoring this evidence vacuum does not eliminate risk.
It merely ensures that risk remains unmeasured, undocumented, and unevenly distributed.
Without coordinated action, clinicians will continue to practice in partial darkness—aware that a variable may matter, yet unable to quantify or manage it appropriately.
That is not conservatism.
It is uncertainty by omission.
Conclusion
Peptides occupy an uncomfortable but unavoidable space in contemporary orthopaedics and sports medicine. They are biologically plausible, widely used by patients, and increasingly relevant to daily clinical practice—yet remain largely outside the boundaries of regulated medicine.
This disconnect is not the result of ignorance, indifference, or resistance to innovation. It is the consequence of a structural mismatch between real-world patient behavior and a regulatory, economic, and research framework that is ill-equipped to address non-patentable, widely used compounds whose primary impact is on public health rather than commercial return.
History suggests that some peptides will ultimately prove beneficial, just as insulin and GLP-1 analogues once did. However, history also teaches that plausibility and popularity are poor substitutes for safety data. Until the necessary scientific steps are taken—and until the barriers preventing those steps are explicitly addressed—clinicians remain constrained by the very safeguards designed to protect patients.
This is not hypocrisy.
It is the cost of practicing responsible medicine within an imperfect system.
Yet responsibility does not end with restraint. It also requires honesty.
When large populations are exposed to biologically active compounds for conditions that are prevalent, disabling, and costly to healthcare systems, ignorance itself becomes a risk. Failing to investigate does not preserve safety; it merely preserves uncertainty—at scale.
Orthopaedics and sports medicine, given their central role in managing pain, inflammation, injury, and degeneration, sit at the epicenter of this issue. The interaction between peptides and surgery, pharmacology, rehabilitation, and orthobiologic treatments is no longer a theoretical concern. It is a clinical reality unfolding without measurement or oversight.
This is precisely the type of problem that demands collective responsibility. When markets cannot justify the cost of research, public health systems, medical societies, and supranational research frameworks must step forward—not to endorse unvalidated therapies, but to illuminate their risks, interactions, and boundaries.
Medicine does not advance by closing its eyes to reality.
It advances by confronting uncomfortable questions—especially when the answers are complex, expensive, and politically inconvenient.
Failing to do so does not delay progress.
It merely postpones accountability—and leaves patients to bear the cost.
Leave a Reply